
{kind=link}
Early intervention for psychosis exhibits promise in altering the outlook for people with schizophrenia spectrum dysfunction (SSD). Early intervention companies for first-episode psychosis (FEP), which is usually outlined as throughout the first 2 to five years of psychotic symptom onset, purpose to offset psychotic signs and related impairment and improve help and abilities to advertise purposeful restoration. Availability of those companies additionally fosters service person engagement with efficient remedy early in the middle of sickness, thereby minimizing the period of untreated psychosis (DUP), as longer DUP is related to poorer long-term outcomes.
Coordinated specialty care (CSC) is a recovery-oriented, team-based, early intervention mannequin. Due to the established effectiveness, the American Psychiatric Affiliation Follow Tips not too long ago thought-about CSC as the usual of look after early psychosis.1 CSC makes use of a phase-specific remedy mannequin comprising evidence-based outpatient companies for FEP to enhance high quality of life, position functioning, symptomatology, and long-term outcomes/prognoses. Whereas CSC applications range, normal parts embody psychotherapy (usually cognitive habits remedy for psychosis or individualized resiliency coaching), medicine administration, household companies (schooling and help), service coordination and case administration, and supported employment and schooling. Peer help was not initially designated as a regular part; nonetheless, many applications now contemplate peer specialists to be important group members.
CSC is among the few psychosocial remedies the US Congress has supported by dedicating nationwide funding to make sure entry to programming. In 2008, federal funds had been allotted to 2 states to help 12 CSC applications. The constructive outcomes of the Nationwide Institute of Psychological Well being’s Restoration After an Preliminary Schizophrenia Episode (RAISE) initiative and subsequent will increase in federal psychological well being block grants put aside funding for FEP contributed to a drastic rise in CSC applications nationally. As of 2023, a complete of 431 CSC applications had been unfold throughout the nation and accessible in each state, per the Substance Abuse and Psychological Well being Companies Administration’s 2023 report. Whereas establishing and rising CSC programming required billions of {dollars} in funding, most research conclude that early intervention applications are cost-effective, given reductions in pricey outcomes and companies (eg, acute care) with compelling cost-related advantages.
CSC Outcomes
CSC has repeatedly yielded numerous remedy positive factors compared with remedy as traditional. Service customers expertise considerably improved functioning (social, occupational, and international) and high quality of life, considerably decreasing scientific signs, suicidality, and fee of hospitalizations.2-5 CSC applications additionally are likely to have excessive retention charges,5,6 a very related consequence for people with SSD, as remedy disengagement is frequent. Along with behavioral outcomes, CSC advantages, resembling improved reward anticipation-associated activation performance and associated buildings related to constructive signs, are additionally obvious utilizing neuroimaging methods.7 In step with CSC’s fundamental purpose, extra vital remedy positive factors are related to decrease DUP and excessive constancy to frequent components of CSC.2,4
TABLE. Ideas for Prescribers
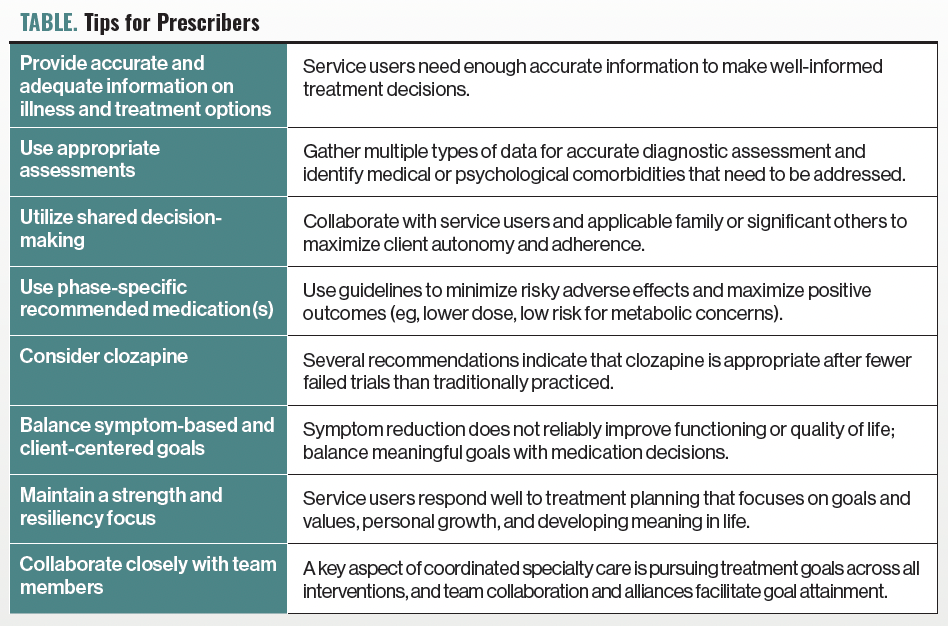
Psychiatrists and different prescribers work collaboratively with different group members and repair customers to implement CSC with constancy. The Desk consists of particular ideas for CSC prescribers which are generalizable to prescribers working with FEP outdoors of CSC. The Schizophrenia Affected person Outcomes Analysis Crew tips8 and publicly accessible NAVIGATE and OnTrackNY manuals are further sources for phase-specific psychopharmacologic suggestions.
Relative Limitations of CSC
Though most CSC contributors profit from programming whereas actively engaged in remedy, fewer long-term postdischarge consequence research have been carried out. An early intervention program outdoors the US carried out a 10-year follow-up research and located higher employment outcomes than normal care.9 Nonetheless, 32% of the early intervention pattern nonetheless represented a “poor employment” cluster. Service customers who obtained early intervention companies made extra employment positive factors than those that obtained normal care. Nonetheless, enhancements deteriorated to the identical degree of functioning as normal care after 5 years. Given this, different vital enhancements might fizzle over time.
Understandably, CSC remedy is time restricted, with most applications providing a 2-year mannequin. Some applications, whereas a minority, present as much as 3 to five years of remedy, and even fewer supply longer postdischarge extensions. Service customers set up robust therapeutic rapport and profit from the great nature of CSC. In the meantime, there’s a important dearth of specialised psychiatric and psychotherapeutic companies accessible for people with SSD locally. For instance, cognitive habits remedy for psychosis (CBTp) is an evidence-based remedy that’s beneficial as the usual of care for people with SSD within the US. Nonetheless, there’s an unbelievable hole in CBTp-trained suppliers within the US to people identified with SSD (roughly 11-22 suppliers for each 10,000 people with SSD).10 Equally, different evidence-based companies, resembling supported employment and household companies, are scarcely accessible. Subsequently, it’s unsurprising that many service customers and clinicians report unreadiness for discharge and hesitation concerning follow-up companies.11
After discharge, service customers are likely to have poor follow-up with outpatient remedy, however charges are elevated with extra months of CSC remedy and fewer relapses earlier than discharge.12 Given remedy period limitations, most service customers, even after your complete period of CSC remedy, proceed to expertise residual signs and purposeful impairment and are susceptible to relapse,13 just like people who weren’t afforded CSC remedy. CSC outcomes show significant positive factors whereas engaged in specialty care, and all people with SSD ought to obtain related, complete remedy. Subsequently, the resource-intensive nature of the CSC method have to be balanced with the fundamental precept that efficient remedy ought to profit all sufferers.
A second limitation is that a lot of the preliminary CSC applications focused nonaffective psychosis, and supplies had been developed for these experiencing signs in line with rising SSD. Nonetheless, early psychosis usually co-occurs with bipolar and depressive problems. Many CSC applications have opted to incorporate people with affective psychosis; nonetheless, CSC information are strongest for nonaffective psychosis, and most manuals and implementation instruments have simply been examined with this inhabitants.
Dialogue
The widespread implementation of CSC has made excellent strides towards enhancing the lives of these with psychosis. With time, extra psychological well being suppliers, together with the authors, marvel, “What about the remainder of our shoppers with SSD?” Entry to specialised, efficient, and complete remedy for people who didn’t obtain CSC-based care or who’ve already been discharged from CSC applications is extremely restricted. Rising the variety of educated psychological well being clinicians working with people with SSD is a well-recognized requirement in pursuing this aspiration. Stimulating curiosity in working with SSD (maybe by persevering with to extend future clinicians’ consciousness of efficient remedies, counter to extensively held misconceptions) and subsequent specialised coaching in CBTp and different evidence-based interventions, resembling abilities coaching, household companies, and well-informed psychopharmacologic practices, would profit this inhabitants.
Psychiatric rehabilitation fashions usually comprise a number of evidence-based remedies for people with SSD. Though efficient, there stays a large science-to-service hole, given the shortage of those applications locally. As with most psychological well being fashions of care, funding/reimbursement regularly hinders implementation. As a product of CSC’s affect on psychological well being care, a team-based billing code was not too long ago established to reimburse CSC-based look after FEP. Contemplating the widespread want, what would it not take to ascertain an analogous billing system to fund complete and specialised applications for all sufferers with SSD (not simply FEP)? Whereas psychiatric and psychological companies are sometimes reimbursable, among the most impactful companies are hardly ever accessible or are usually not adequately reimbursable (eg, supported employment, household companies, peer help). Additionally, CSC applications have variable and sometimes strict eligibility standards (eg, age, time since onset, insurance coverage standing), which might result in frustration and disappointment amongst service customers, households, and clinicians. Moreover, many CSC applications are properly beneath service capability,14 so maybe some applications may use funds for flexibility and longer-term look after these in want.
Concluding Ideas
CSC has reworked psychological well being look after psychosis and recalibrated the sphere’s outlook on restoration. The restoration orientation and multicomponent mannequin usually meet the wants of people with SSD who usually expertise demoted autonomy with cross-domain impairment. Implementing CSC has vastly improved essential outcomes for service customers and regularly lessens the pricey burden of high-cost psychological well being care. Early intervention for SSD would profit from extra long-term consequence research to additional illuminate variations in sickness trajectory. Numerous people would profit from taking the teachings discovered from CSC to use them to psychological well being care for people previous the primary episode of psychosis, the vast majority of the inhabitants with SSD.
Dr Warner is an affiliate professor of psychiatry and behavioral sciences on the College of Texas Well being Science Heart at Houston. Dr Glynn is a analysis psychologist on the College of California, Los Angeles. Dr Hong is an endowed professor of psychiatry and behavioral sciences at The College of Texas Well being Science Heart at Houston.
References
1. Keepers GA, Fochtmann LJ, Anzia JM, et al. Assessment of analysis proof supporting guideline statements. The American Psychiatric Affiliation Follow Guideline for the Therapy of Sufferers With Schizophrenia. Third version. American Psychiatric Affiliation Publishing; 2020.
2. Hazan H, Tayfur SN, Zhou B, et al. The affect of period of untreated psychosis on functioning and high quality of life over one 12 months of coordinated specialty care (CSC). PLoS One. 2025;20(2):e0312740.
3. Phalen P, Jones N, Davis B, et al. Suicidality amongst shoppers in a community of coordinated specialty care (CSC) applications for first-episode psychosis: charges, modifications in charges, and their predictors. Schizophr Res. 2024;274:150-157.
4. Rosenblatt A, George P, Ghose SS, et al. Constancy to frequent components of coordinated specialty care: outcomes of shoppers with first-episode psychosis. Psychiatr Serv. 2024:appips20230548.
5. Robinson DG, Schooler NR, Marcy P, et al. Outcomes throughout and after early intervention companies for first-episode psychosis: outcomes over 5 years from the RAISE-ETP site-randomized trial. Schizophr Bull. 2022;48(5):1021-1031.
6. Kane JM, Robinson DG, Schooler NR, et al. Complete versus traditional neighborhood look after first-episode psychosis: 2-year outcomes from the NIMH RAISE early remedy program. Am J Psychiatry. 2016;173(4):362-372.
7. Smucny J, Lesh TA, Niendam TA, et al. Proof for purposeful enchancment in reward anticipation in current onset schizophrenia after one 12 months of coordinated specialty care. Psychol Med. 2023;53(13):6280-6287.
8. Kreyenbuhl J, Buchanan RW, Dickerson FB, Dixon LB. The Schizophrenia Affected person Outcomes Analysis Crew (PORT): up to date remedy suggestions 2009. Schizophr Bull. 2009;36(1):94-103.
9. Chan SKW, Pang HH, Yan KK, et al. Ten-year employment patterns of sufferers with first-episode schizophrenia-spectrum problems: comparability of early intervention and normal care companies. Br J Psychiatry. 2020;217(3):491-497.
10. Kopelovich SL, Nutting E, Clean J, et al. Preliminary level prevalence of cognitive behavioral remedy for psychosis (CBTp) coaching within the U.S. and Canada. Psychosis: Psychological, Social and Integrative Approaches. 2022;14(4):344-354.
11. Jones N, Gius B, Daley T, et al. Coordinated specialty care discharge, transition, and step-down insurance policies, practices, and issues: employees and shopper views. Psychiatr Serv. 2020;71(5):487-497.
12. Hyatt A, Mullin B, Hasler V, et al. Predictors of relapse and engagement in care one 12 months after ending companies in an city security web coordinated specialty care program for first episode psychosis. Schizophr Res. 2023;264:140-146.
13. Chang WC, Kwong VWY, Lau ESK, et al. Sustainability of remedy impact of a 3-year early intervention programme for first-episode psychosis. Br J Psychiatry. 2017;211(1):37-44.
14. George P, Ghose SS, Goldman HH, et al. Development of coordinated specialty care in america with modifications in federal funding insurance policies: 2014–2018. Psychiatr Serv. 2022;73(12):1346-1351.